Legislation and Legislative History
- The original, National Organ Transplant Act of 1984 (public law 98-507, i.e., 98th Congress, 507th law passed)
- excerpts from accompanying U.S. Senate report
- list of U.S. Senate sponsors of the 1984 legislation
- list of U.S. House sponsors of the 1984 legislation
- U.S. House testimony in favor of the ban
- U.S. House testimony in opposition to the ban
- Pennsylvania's proposed organ-donor funeral reimbursement plan
Scientific Articles
- Journal of Transplant Coordination (1999):"Willingness to donate organs and tissues in Vietnam", by Tran Bac Hai et al.
- Issues in Medical Ethics (IX(2): 44-46, April-June, 2001): "The Ethics of Organ Selling: A Libertarian Perspective", by Harold Kyriazi [yours truly]
- Journal of Medical Ethics (27: 30-35, Feb. 2001): "Shifting ethics: debating the incentive question in organ transplantation", by Donald Joralemon [Editor's note: this article, available on-line, provides a reasonably unbiased analysis of the debate, and has tons of good references, both pro and con]
Press Articles
- David Rothman's "The International Organ Traffic"
- Insight magazine's 1992 cover story, "The Organ Brokers"
- "Transplanting Life: The
Triumphs, The Traps, The Tragedies."
A Five-Part Series by The Plain Dealer - San Diego Union-Tribune article about one donor and her many recipients, "Of death and life"
- Dear Abby column
- CATO Institute column (this is on an adjacent page)
- AMA reconsidering the ban on selling (at June, 2002 meeting)
- AMA recommends experimenting with monetary incentives (June 2002)
- UCLA law professor recommends monetary incentives for cadaveric donation (October 30, 2005)
ABC News' 20/20, John
Stossel report, "Organs for Sale? With So Many People in Need
of Organs, Why Can't They Buy Them?" (August 8, 2003)
CBS News'
48 Hours Special ("Your Money or Your Life" -- first aired
Monday, Feb. 11, 2002)
An Inspirational Poem (from the mother of a donor)
"Willingness to donate organs and tissues in Vietnam" by Tran Bac Hai, Ted Eastlund, MD, Le Anh Chien, Phan Thi Hong Duc, Tran Huong Giang, Nguyen Thi Nguyen Hoa, Phan Hong Viet, and Duong Quang Trung, MD, Journal of Transplant Coordination 9(1): 57-63 (1999). The following quote is from p. 62: "We observed that many families preferred to receive monetary or other material inducements for donating organs or tissues from deceased family members." [Straight from the horse's mouth! And why shouldn't they receive some compensation, as a small token of gratitude?]
David Rothman's New York Review of Books article, "The
International Organ Traffic" (The New York Review, March 26, 1998)
"The market in organs has its
defenders. To refuse the sellers a chance to make the money they need, it is said, would
be an unjustifiable form of paternalism. Moreover, the sellers may not be at greater risk
living with one kidney, at least according to US research. A University of Minnesota
transplant team compared seventy-eight kidney donors with their siblings twenty years or
more after the surgery took place, and found no significant differences between them in
health; indeed, risk-conscious insurance companies do not raise their rates for kidney
donors. And why ban the sale of kidneys when the sale of other body parts, including
semen, female eggs, hair, and blood, is allowed in many countries? The argument that these
are renewable body parts is not persuasive if life without a kidney does not compromise
health. Finally, transplant surgeons, nurses, and social workers, as well as transplant
retrieval teams and the hospitals, are all paid for their work. Why should only
the donor and the donor's family go without compensation?"
 From the 1998
David Rothman, NY Review article. Note the long abdominal scar. (It looks a bit like she
has a rope around her waist.)
From the 1998
David Rothman, NY Review article. Note the long abdominal scar. (It looks a bit like she
has a rope around her waist.)
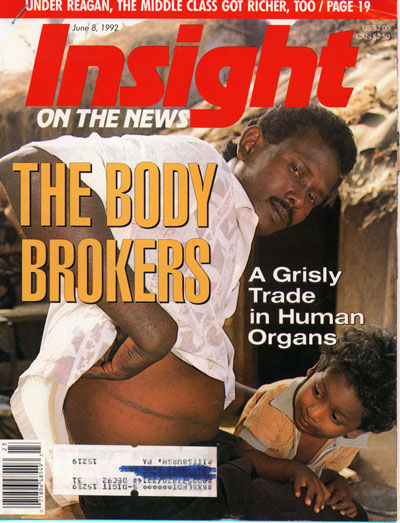
June 8, 1992 Insight magazine cover story.
Body Shops, by Stephen Brookes
Squatting in a dirt alley in the Indian slum of Villivakkam, the slight
young man pulls up his shirt and runs his finger along the rough, 8-inch scar that erupts
below his rib cage and runs down his abdomen into the folds of his skirt-like lunghi.
"This is where they cut me open to get the kidney out," he murmurs,
describing the operation he underwent in a Madras hospital three years ago.
"They paid me 20,000 rupees (about $800) for it, half before and half after.
It's all gone now," he says, laughing self-consciously. "I had a lot of
debts, and I drank the rest. I was stupid, and now I'm sick. I can't even work
anymore. I'm 27 years old, and if I carry a bucket of water down the street I have
to sit down and rest."
It's a story that's becoming increasingly familiar across India, Latin
America and other parts of the developing world: poor people recruited from slums and
shantytowns to sell parts of their bodies for quick cash. The buyers: wealthy
Japanese, Middle Easterners and Europeans who, frustrated with laws against buying organs
in their home countries, go abroad to countries where they can check into a hospital, find
a middleman to procure a donor, pay for the transplant and return home - all in a matter
of weeks. "The practice is apparently widespread, from what we've been
hearing," says an official with the World Health Organization in Geneva.
"And we're very concerned."
The concern is warranted. With kidneys selling for anywhere from
a few hundred to tens of thousands of dollars, the trade has become so lucrative that
there have been reports - some substantiated, some questionable - of children in Argentina
being stolen and killed for their organs, of Chinese prisoners executed and their kidneys
sold, of prisoners in the Philippines being released after donating a kidney, of bodies
washing up on Brazilian beaches with their organs surgically removed. At one
psychiatric clinic outside of Buenos Aires, Argentina, doctors have been accused of
murdering lunatics for their body parts. Large, well-organized trafficking rings
have even been uncovered: in December, Juan Andres Ramirez, Interior Minister of Uruguay,
announced the arrest of 20 persons who were allegedly flying slum dwellers to other
countries to "donate" their organs.
While some of the stories are patently untrue - widespread reports in
the early 1980s that Latin American children were being stolen and their organs sold to
rich Westerners, for example, were later shown to be part of a bizarre Soviet
disinformation campaign - there are thriving, well-documented and quite legal markets in
Bombay, Madras and Calcutta in India, and in Manila, Cairo and Hong Kong. Many of
the buyers are nationals, but much of the trade is fueled with oil money from outside.
"Most of the buyers are coming from the Emirates, Qatar and Kuwait," says
the World Health Organization official, describing the kidney business in Cairo and
Bombay. "Apparently there's a big shortage of kidneys in the Gulf states right
now, because of the war."
The growth of this grisly trade has resulted from two related trends
over the past two decades. On the one hand, medical and technological developments
have raised the success rate of transplants and increased the demand for organs; but as
demand has gone up, laws have been implemented in most of the world forbidding people to
pay organ donors, thus cutting down the potential supply. That imbalance has spawned
a complex network of desperate buyers, shady middlemen, opportunistic doctors, and poor
and uneducated donors.
While corneas, lungs and other organs can be transplanted from live
donors, most of the trade is in kidneys, since a healthy, well-nourished donor can live
reasonably well with only one. Since the first renal transplant was done in 1954
between twin brothers, the survival rate has gone up dramatically, thanks to advances in
surgical techniques, the training of large numbers of transplant surgeons and the
development of drugs such as cyclosporine that suppress immune system attacks on
transplanted organs. For patients who suffer from chronic kidney failure, there is
now greater hope that they can be released from the expensive, endless and intrusive
mechanical process of dialysis (which cleanses impurities from the blood) and live a
normal life with a transplant.
But finding a donor is not easy. Successful transplants rely on a
good blood and tissue match between donor and recipient, and the best donors are often
members of one's family. But patients who lack a willing family member have only two
choices: wait until a properly matched kidney from a cadaver becomes available or go to
one of the world's kidney marketplaces.
Until a few years ago it was possible in the United States and Europe
to bring donors in from outside. As early as 1985, the World Medical Association
noted that "in the recent past a trade of considerable financial gain has developed
with live kidneys from underdeveloped countries for transplantation in Europe and the
United States."
But as more and more such cases came to light, governments began to
respond. Washington outlawed trade in body parts with the National Organ Transplant
Act of 1984 - sparked by the revelation that a doctor in Virginia had circulated brochures
in the Caribbean, offering people a free two-week vacation in the United States if they
agreed to leave a kidney behind when they went home.
Other Western governments soon followed suit.
... In one notorious 1988 case, a German company called the Association
of Organ Donations and Mutual Human Substitution sifted through public bankruptcy notices
to find prospective clients, then sent them a letter that read, "You're broke.
You're a social leper, tainted with the legal and social equivalent of AIDS. The
most horrid vultures will pursue you. ...In case you don't have the guts for a life of
crime, if your courage isn't up to a big break-in, a bank heist or a new life abroad, I
offer you a solution founded on logic. Donate your kidney."
The founder of the company, Count Rainer Rene Adelmann von
Adelmannsfelden, offered to pay up to $45,000 for kidneys and to arrange operations -
including doctor, donor and hospital fees - for $85,000, taking a 10% cut for himself. ...
Nor is Asia spared. Japanese suffering from kidney disorders
are said to flock to Manila for transplants, while wealthy residents of Hong Kong and
Singapore reportedly cross the Hong Kong border into Guangzhou in southern China.
According to Hong Kong doctors and human rights groups, an organization
calling itself the Kidney Transplant Service Center has offered package tours to China for
kidney transplants, and a prominent Hong Kong doctor told the British medical journal
Lancet recently that customers pay about $20,000 for a kidney transplant.
But there have also been more sinister
reports of transplants done at Nanfang Hospital in Guangzhou, in which prisoners
were executed and their organs removed for sale to foreigners (at a going
rate of $10,000 to $13,000) or high Chinese officials. The details were confirmed
by a Chinese police official, who told the International League for Human Rights that
"those who were executed would have their organs removed for transplant without prior
consent or that of their families. For example, a colleague of mine who was going
blind took the eyes of a prisoner who was executed. In order to
preserve the eyes, the prisoner was shot in the heart rather than in the head. This
is what happens. If they need the heart, the prisoner would be shot in the head
instead."
When asked who would actually remove the organs, the police official
said a doctor and a nurse would arrive in an ambulance. "Immediately after the
execution, the coroner would examine the corpse and certify the death. The corpse
would then be taken immediately inside the ambulance, where the necessary organs are
removed. The corpse is then taken out of the ambulance and returned to the family.
No one has seen the doctor or nurse, and no one is aware of the reason why they
were there."
While the trade thrives in China, Hong Kong and the Philippines, it is
also strong in the Middle East. ...
While a poor man can make a few thousand dollars, it's the middlemen -
the people who bring foreign buyers and sellers together - who really profit. One
such middleman, who agreed to talk anonymously about his business, met with
Insight late one night on a side street on the outskirts of Cairo. A
smooth-talking operator, fluent in English, French and Italian as well as his native
Arabic, he wore expensive European clothes, chain-smoked Gauloise cigarettes and sat in
the backseat of a gold Mercedes as he described some of the kidney transplants he had
arranged. "It's very simple, and it happens all the time," he says.
"The first one was in 1987. I was working at the Sheraton el-Gezira, and there
was a guest staying there, a Kuwaiti. He'd been asking around about finding someone
who would sell their kidney, and I went up to see him. He was about 30. He
said he'd made arrangements for the operation, but had to find a donor. And he said
he'd pay $9,000.
"So I got in touch with my brother, who's a soldier in the Seqoa
Oasis. He had a houseboy there, a Bedouin. He was about 20, I think. He
agreed to come up to Cairo, they did the blood tests, and they did the operation a few
days later." In all, he says, there were six persons involved: the seller, the
donor, himself, the doctor and a couple of nurses. "The Kuwaiti paid $29,000
for everything. I got $7,000. The Bedouin got $2,000, and the rest went to the
doctors and the nurses. The Kuwaiti went back home, and about six months later I got
a call from a friend of his, another guy who needed a kidney. It's a good
business," he says, sitting back in the Mercedes and smiling.
If business is good in Egypt, it's even better in India. ...
Supply & Demand [sidebar]
As the demand for kidneys shoots up, is there any way to increase the
supply without legalizing a live donor market? In the United States and other
developed countries, the technology exists to remove kidneys from cadavers, freeze them,
match them to a potential recipient through a centralized directory and then quickly
deliver them. Under the Uniform Anatomical Gift Act, people can authorize the
postmortem donation of their organs, and in most states people can indicate on their
driver's licenses if they are willing to let their organs be removed for transplanting.
Yet in spite of encouragement from doctors, the government and some
religious leaders, many people simply refuse. There are some 15,000 to 25,000 deaths
of healthy people in the United States every year, but only about 20 percent of those
result in donations, leaving the supply far short of the 13,000 to 15,000 kidneys needed
every year.
"The harsh reality is that, with respect to cadaver donation,
you're never going to get enough to meet demand," says Arthur L. Caplan, a medical
ethicist at the University of Minnesota.
Caplan and others believe that while the debate on allowing people to
sell their organs may heat up in the future, there are so many complex practical and
ethical issues involved that the laws are unlikely to change.
The organ shortages of the future will probably be met by other means,
they say: Xenografting - or transplanting animal organs into humans - remains a promising
solution, and the use of mechanical devices to replace certain organs is also developing.
And as biotechnology develops, it may eventually be possible to grow
whole organs from a few cells - making test tubes the organ donors of the future. [end
sidebar]
[The article is long, and continues to document the horrors of the trade. I can't help but note the similarity between this and the trade in illegal, recreational drugs, where the government "solution" is a hundred times worse than the perceived problem. Reagan was largely correct when he said, "Government isn't the solution. Government is the problem."]

Dear Abby
by Abigail Van Buren
From the San Diego Union-Tribune, Sunday, January 23, 2000
[Responding to a tax attorney who wrote, "I am not in support of the person who suggests that we give incentives to encourage people to become organ donors. The incentive should be that you are doing the right thing for the right reason. There is no other incentive necessary."]
Dear Mr. ___: ... I agree with you that no incentive other than doing the right thing
for the right reason should be necessary.
However, at this time 66,717 people are on organ-donor waiting lists,
praying for a heart, a kidney or a liver that will save their lives. Last year,
4,800 people died while waiting for that prayer to be answered. Is it
more immoral for someone to die because there is a shortage of organs available, or to
offer tax incentives to those who would otherwise bury their dear departed, organs and
all?
I found this on Dear Abby's web site (2/8/00)
DONOR'S MOTHER FINDS HOPE IN LINKING LIVING WITH DYING
DEAR ABBY: In 1989, my nephew Bryan and his fiancee were killed in an automobile accident.
He was only 21 years old. My brother-in-law and sister were faced with that dreaded
question, "Is your son an organ donor?" In fact, he was, and had discussed his
wishes with his parents some time before the accident. As a result of Bryan's
unselfishness, several people's pain was ended and their bodies were mended.
A couple of years later, my sister was asked by a nurse who worked in transplant services
to speak to a group of medical professionals who deal with organ donation and donor
families. She was told that they never had a problem getting a recipient to come and tell
the story from that point of view, but it was rare to find a donor mom or dad who would
discuss how being approached for donation had affected their lives and what it meant to
them.
Those people wanted to know how she felt about what took place in that drab little room
off to the side of the emergency room on the night her son died. They knew they would be
faced with asking that question again and again, and wanted to know if she could give them
a word of encouragement or correction to make them better equipped to help the next
family. How could she refuse?
In the days to follow she wrestled with the thought of standing in front of a group of
strangers and pouring out the horrible story. She decided she needed to jot down something
that could be read for her in case she fell apart. In the space of an hour, the enclosed
poem is what God's grace allowed her to express. Perhaps you will feel it's worth sharing
with your readers. -- RON BELSHE, RICHARDSON, TEXAS
DEAR RON: I offer my condolences for the tragedy that took your nephew and his fiancee.
Your sister's poem is certainly worthy of space in this column. Read on:
DON'T GIVE UP
by Becky Hanson
If you can swallow hard enough to push away the fear,
And say yes to the question that no one wants to hear,
Then you will add a ray of hope when there's nothing left but crying,
And become the "gentle link" between the living and the dying.
I believe that you'll find comfort though your heart has been laid raw,
In offering hope to someone else who prays and waits in awe.
Until it's done, you can't know how or whom your words will bless,
But hundreds more will find new life if you will answer "yes."
By Bruce Japsen (Chicago Tribune staff reporter)
June 19, 2002
With 16 people dying every day for lack of a needed organ, the American Medical Association on Tuesday said it would support studies to determine whether money should be used to motivate potential donors and their families.
Although the AMA's decision is only a baby step toward financial payments for organ donation, the vote by the nation's largest doctor group is nevertheless significant, organ banks said. Just six months ago, the AMA's policymaking House of Delegates turned down a similar measure at its winter meeting in San Francisco.
This time, however, supporters of the measure were able to convince enough AMA delegates that the lack of available organs is, indeed, a crisis, and merely studying financial incentives could at least help medical professionals and lawmakers understand what drives donations.
Congress banned such financial incentives in 1984, leaving patients who need organ transplants to a volunteer system the AMA and other medical professionals admit has failed.
Nearly 6,000 Americans--an average of 16 a day--die each year as the waiting list for organs surpasses 75,000, a fivefold increase from the late 1980s.
"In a perfect world, altruism would be the answer, but we are not in a perfect world and all of the things we have tried to do haven't worked," said delegate Dr. Phil Berry, a Dallas orthopedic surgeon who had a liver transplant in 1986.
Berry said he was one of the lucky ones, receiving a liver donated from a woman who had died of a bleeding aneurysm. Berry had contracted hepatitis B from a patient during a 1983 surgery just four months before a vaccine became available for the disease.
"I feel so sorry for the 6,000 people who die every year and we need to look into anything that might help them," Berry said. The studies would only look at payments to the families or estates of patients who are dying. AMA policy forbids financial incentives paid to living donors.
Although the AMA itself wouldn't conduct pilot studies, the organization said it would help guide them so they meet ethical and scientific standards. The AMA said such studies, which don't exist, should be done by organ procurement agencies and transplant centers.
"The AMA is not endorsing the use of financial incentives to increase organ donation; it is simply recommending that this concept be studied," said Dr. Frank Riddick, chairman of the AMA's Council on Ethical and Judicial Affairs. "Financial incentives should be of modest value."
Among the incentives the AMA debated included tax credits or payments of $500 to $1,000 toward funeral expenses incurred by the donor family. A bill in Congress looking at ways to increase organ donation would provide a tax credit of up to $10,000 to the estate of an organ donor.
But opponents of incentives say paying donors is unethical and could dilute the altruistic motivation of donors.
"Financial incentives have the potential to exploit poor people," said Dr. Michelle Petersen, an Omaha physician from the eight-member Nebraska delegation, which opposed the effort backed by the AMA on Tuesday. "This promotes [selling] of the human body, reducing all of us as parts for sale. This is not ethical."
Doctors say most organ donations today are made at the last minute by families of people who have died unexpectedly. In such instances, many families decline to sign off on a donation.
Organ banks say the AMA's move will at the very least increase attention to the organ donation crisis.
The non-profit Regional Organ Bank of Illinois said it welcomed the AMA's support of the study.
"If this is going to increase organ donation, then it is something we would support," said John Valencia, the organization's spokesman.
"We don't know whether a study is going to be a positive or a negative," Valencia said. "The fact that this has been publicized may motivate people to donate."
Copyright © 2002, Chicago Tribune
Russell Korobkin's Oct. 30, 2005 Los Angeles Times Commentary
"Sell an organ, save a life
Compensation for donations? It's one way to help those on transplant waiting lists.
"
RUSSELL KOROBKIN is a UCLA law professor and a faculty associate at the UCLA Center for Health Policy Research.
ACCORDING TO RECENT reports, doctors at St. Vincent Medical Center in Los Angeles improperly transplanted a liver into a patient who was not at the top of the applicable waiting list. One person died who should have received the liver and didn't; one person lived by jumping the queue and receiving a liver to which he was not entitled. This is a scandal, but a small one. The far larger scandal is that thousands die every year waiting for transplants in this country because of a misguided government policy.
Nearly 90,000 people are on waiting lists for organs in the United States, most hoping for a kidney or a liver, fewer in need of a heart or a lung or a pancreas. Time runs out for about 6,500 each year.
Only a small percentage of deaths occur in ways that yield organs useful for transplants. Even so, if all those organs were harvested, there would be enough to provide transplants for most of those who die waiting. One important reason for the shortfall is that federal law prohibits donors or their families from receiving any compensation for donations.
The law — the National Organ Transplant Act — is based on the perfectly pleasant idea that organ donations should be altruistic. Unfortunately, the reality is that most of us are not very altruistic. Only a minority of Americans put the tiny "donor" sticker on driver's licenses or otherwise sign up to allow organs to be harvested and transplanted. Absent such prior assent, doctors are often reluctant to ask permission from the next of kin, and, when they do, the next of kin often refuse.
Some who choose not to be donors have a deep personal objection, religious or otherwise, to organ donation. Most people, however, fail to provide assent to donate because they don't want to confront their mortality. And why should they, when there is nothing in it for them or their families? It is much easier just to ignore the issue.
Surely the shortage of organs for transplant could be alleviated if the law were changed to allow modest payments for harvestable organs of the deceased. A system for providing incentives could be organized in many different ways.
The government could give a small tax break, perhaps $20 off driver's license renewal fees, to anyone who agrees to have organs harvested after death. The amount would be small because the organs may not be suitable for transplant. Alternatively, once a person has died, and doctors know that his organs are suitable, the next of kin could be paid a larger amount, perhaps a few thousand dollars, for the right to use those organs. The few who actually object to donating their organs can decline the inducements, while the many who have no strenuous objection will have an incentive to do the right thing.
Where would the money come from? The costs could be passed along to recipients, or more likely their insurance companies, Medicare or Medicaid. Transplant surgeries already cost tens or even hundreds of thousands of dollars (hospitals, doctors and other transplant service providers are legally permitted to make money on organ transplants), so paying for organs and administering such programs would not increase the total cost of transplants appreciably.
Two common objections to permitting payment for organs are that the poor would be disproportionately likely to sell their organs and then suffer ill health effects, and that the rich, who could best afford to pay for organs, would disproportionately benefit. But both of these pitfalls are easily avoided.
First, compensation should be permitted only for organs of the deceased. As long as the living are not paid for a kidney or a portion of a liver, there is no reason to fear a coercive organ market. In fact, such a policy could drastically reduce the number of Americans and other Westerners who, in desperate need of a transplant, travel to Third World countries where they can receive organs sold by living donors.
Second, organ procurement should remain separate from organ allocation. The government or transplant centers should act as the purchasing intermediary and continue to allocate harvested organs according to factors such as medical need, likelihood of a successful transplant and time spent on a waiting list.
Current law pays an unacceptably high price to indulge the moral intuition that human organs should not be bought and sold. The law should be more concerned with saving the lives of thousands who die needlessly.